Sharkfin

TLDR
There is a tricky situation where massive ST elevation can lead to an unclearly defined ST segment. This can EASILY be mistaken for a RBB by computer and physician alike. Best described as a "sharkfin" appearance the diagnosis is further aided by a technique where segments in well differentiated leads can be measured then superimposed on a sharkfin to reveal it's true colors.
Easy to miss. Impossible to forget.
This is an ecg pattern that you have to have exposure to because it will invariably swim into your ED one day and you can bet money the computer read of the tracing will do it's best to reassure you that it's nothing to worry about. Lets take a quick look at the case.
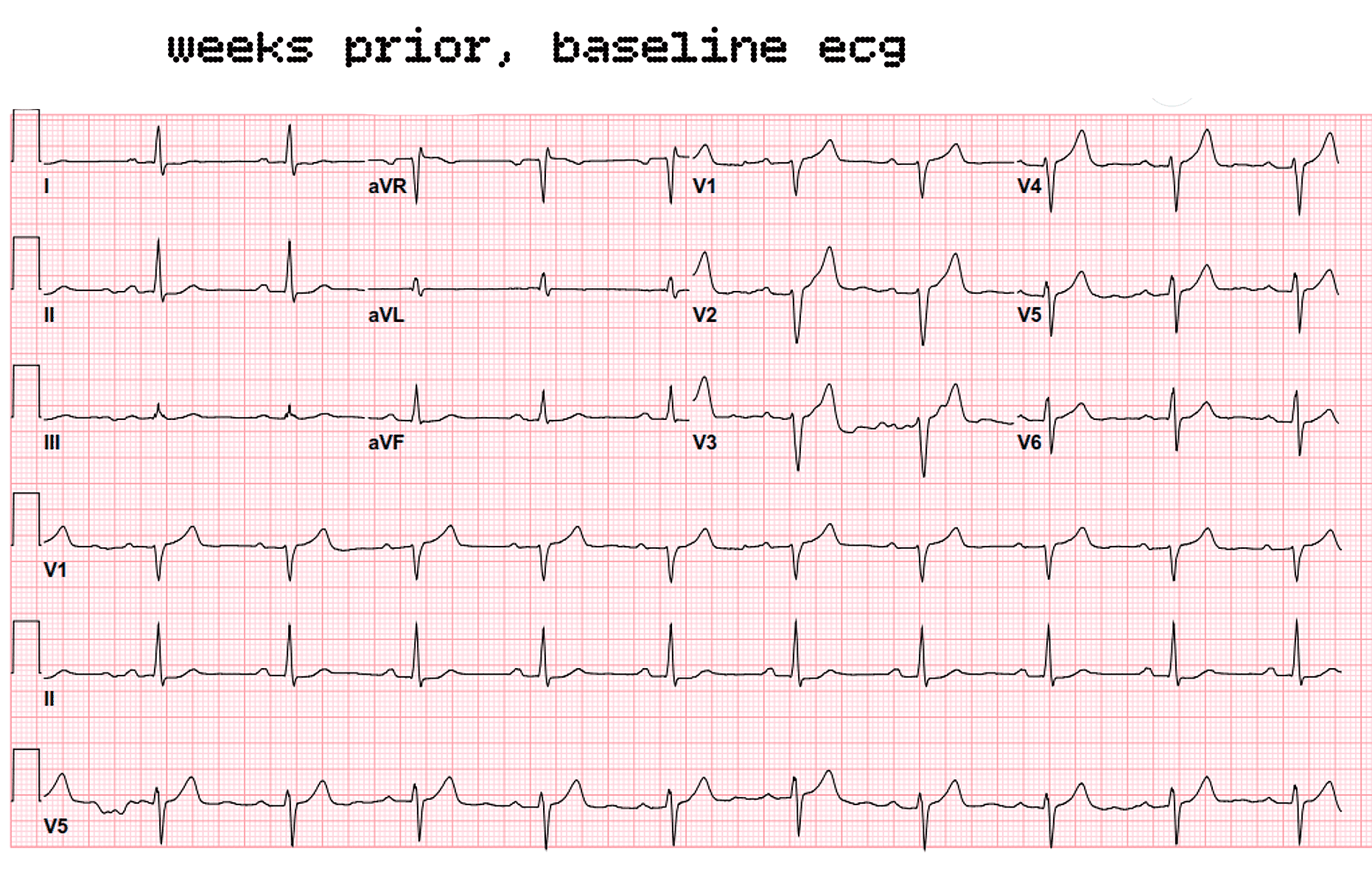
First the baseline ecg from a few weeks ago. Click to enlarge. ESC to return.
Hidden in plain sight
Patient presented to the ED and coded shortly afterwards. Lets have a look at all the ecg tracings in sequence before discussing them in too much detail. While looking over use this checklist:
1 . Where is the shark fin?
In simple terms explain why this is not a RBB and is STEMI.
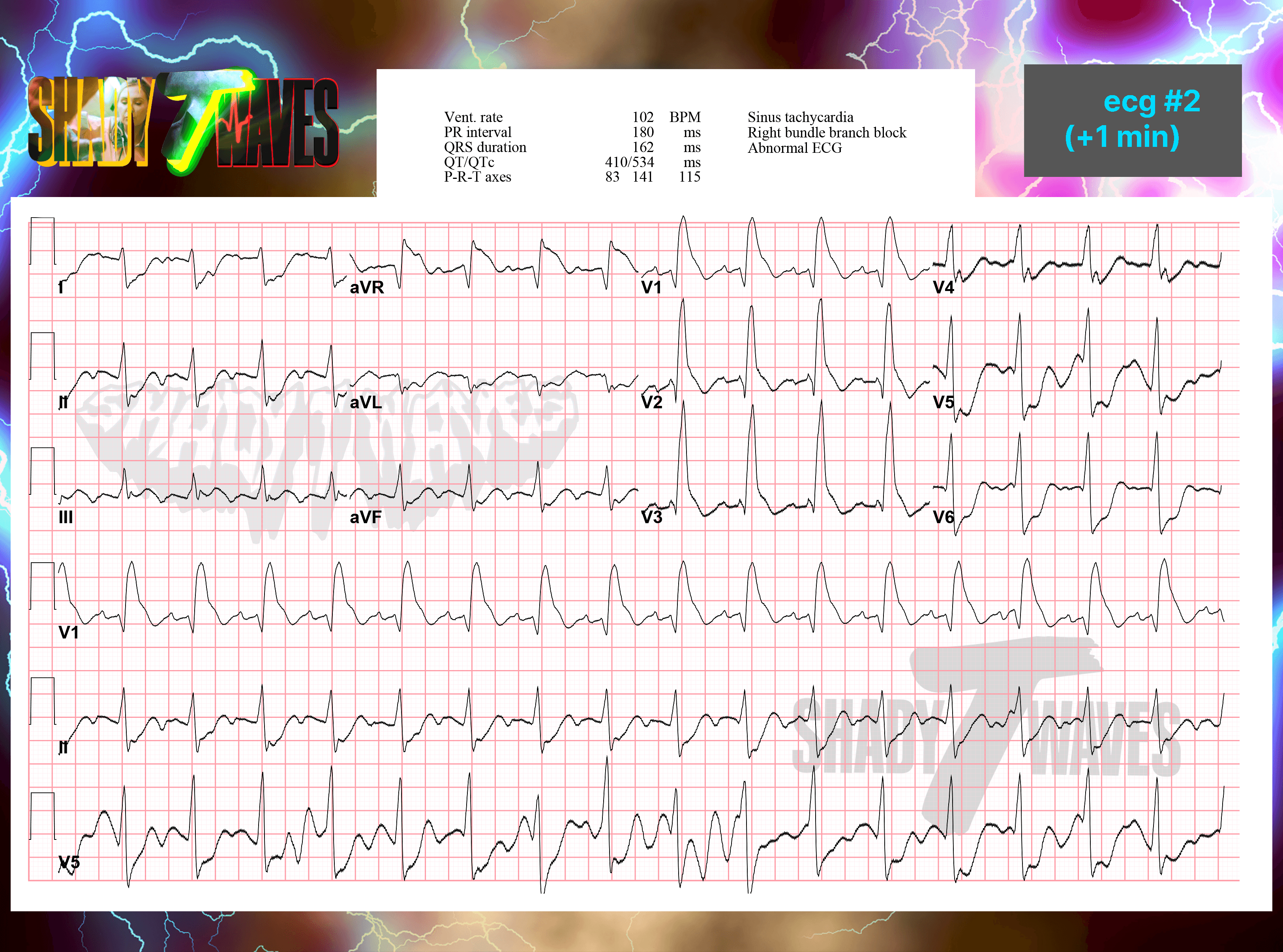
A second tracing captured a minute after the first. (Click to enlarge. ESC to return.)
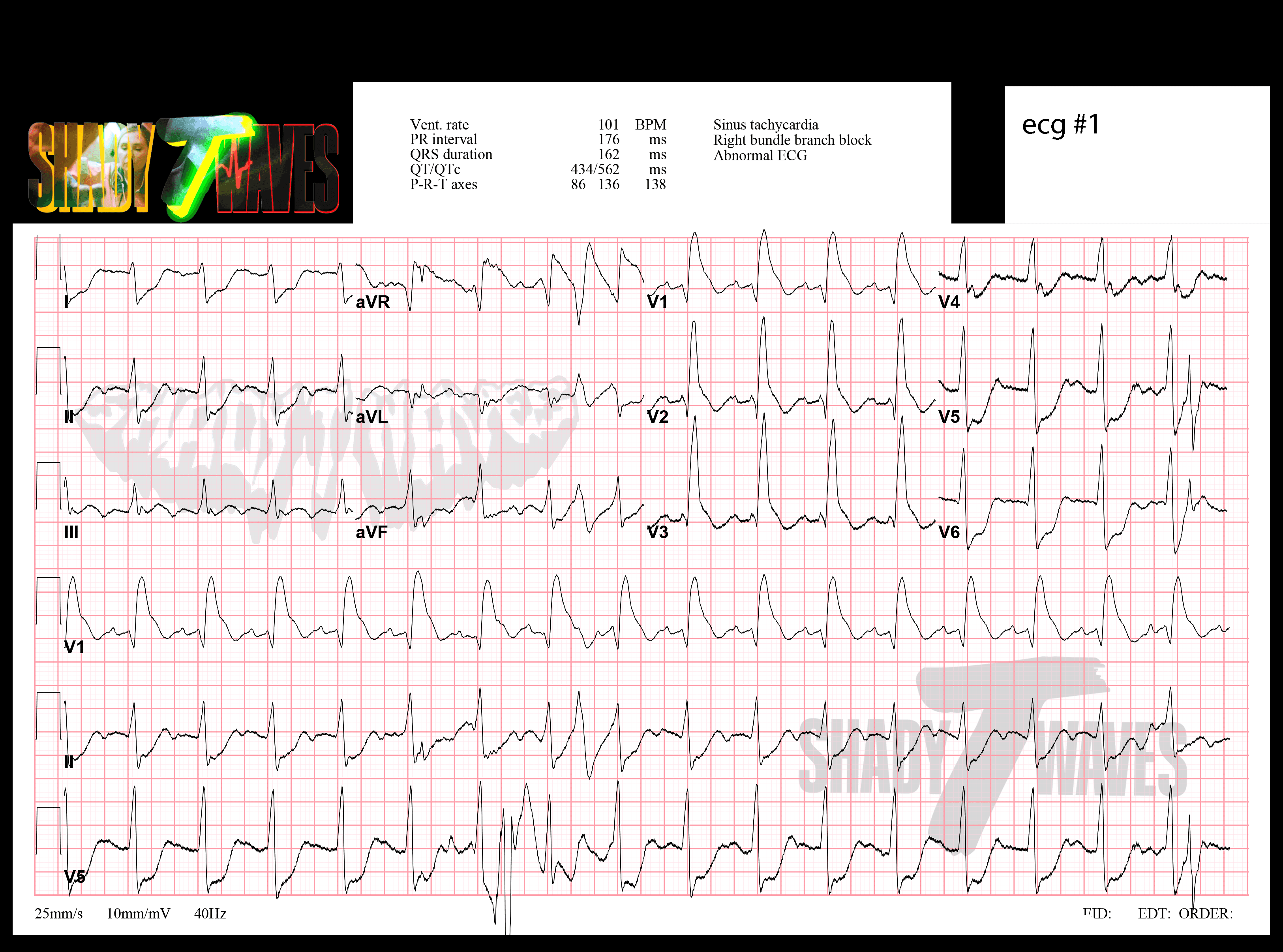
Initial ECG. Pt quickly coded upon entering the ED. (Click to enlarge. ESC to return.)
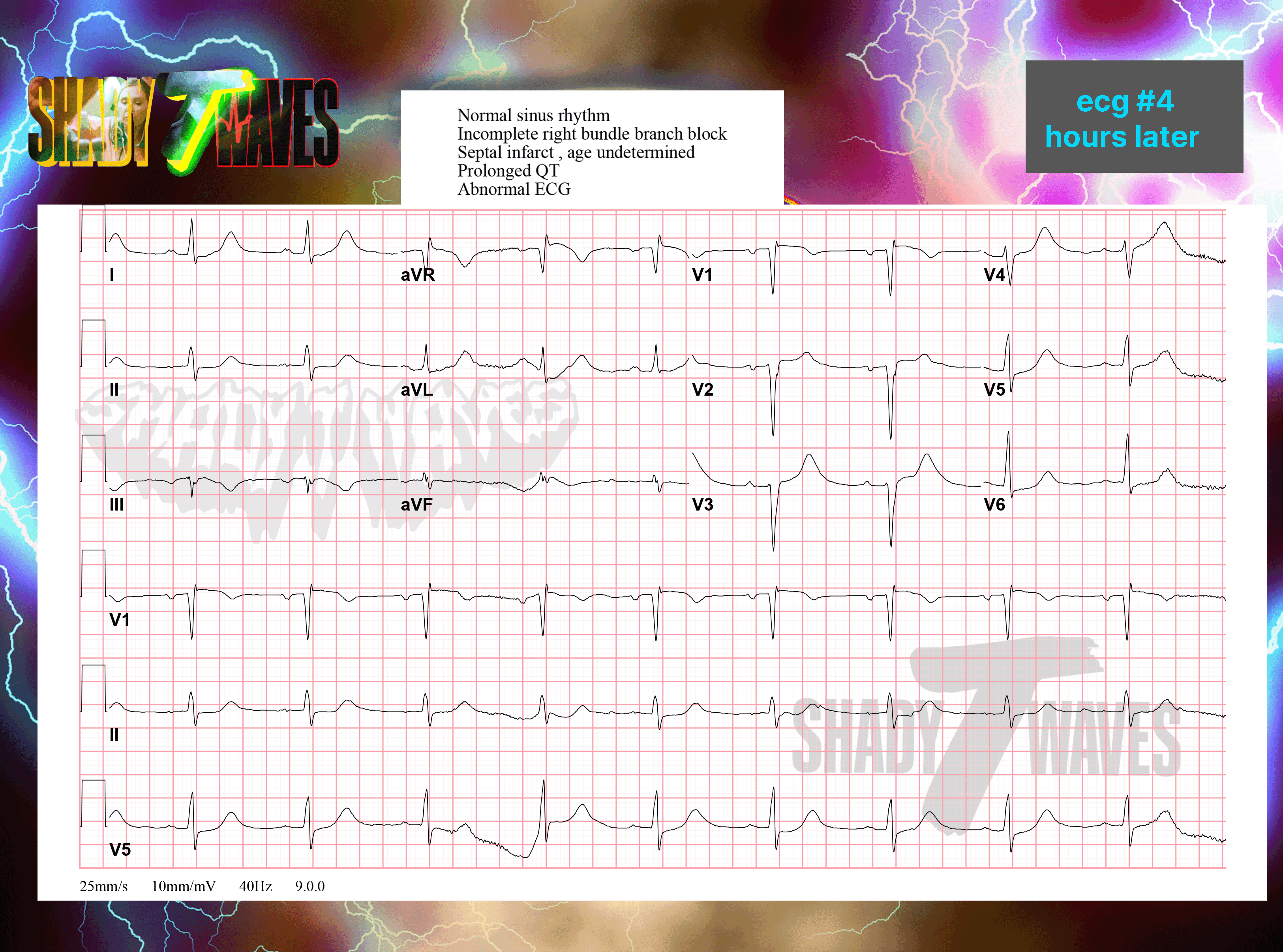
A final tracing obtained some hours after tpa administration. (Click to enlarge. ESC to return.)
Sharkfin Soup
When facing an odd looking RBB consider STEMI. Also consider hyperkalemia or in some situations VT as well. Also notice how the computer does it's best to reassure you that nothing is the matter here. This is the case in all the cases I have had or those shown to me by colleagues.
Although the RBB in these ecgs might feel a little "off" you really need to be able to clearly and simply explain it to a colleague, the interventionalist, or with enough confidence to pull the trigger on lytics as in this case. Just recognizing something is off about the pattern can be helpful but it is even more helpful to use a tried and true method.
Below is is the strategy I have come up with that best works and I have seen the same described on various other websites—if there is any other tricks please leave a comment so I can learn them.
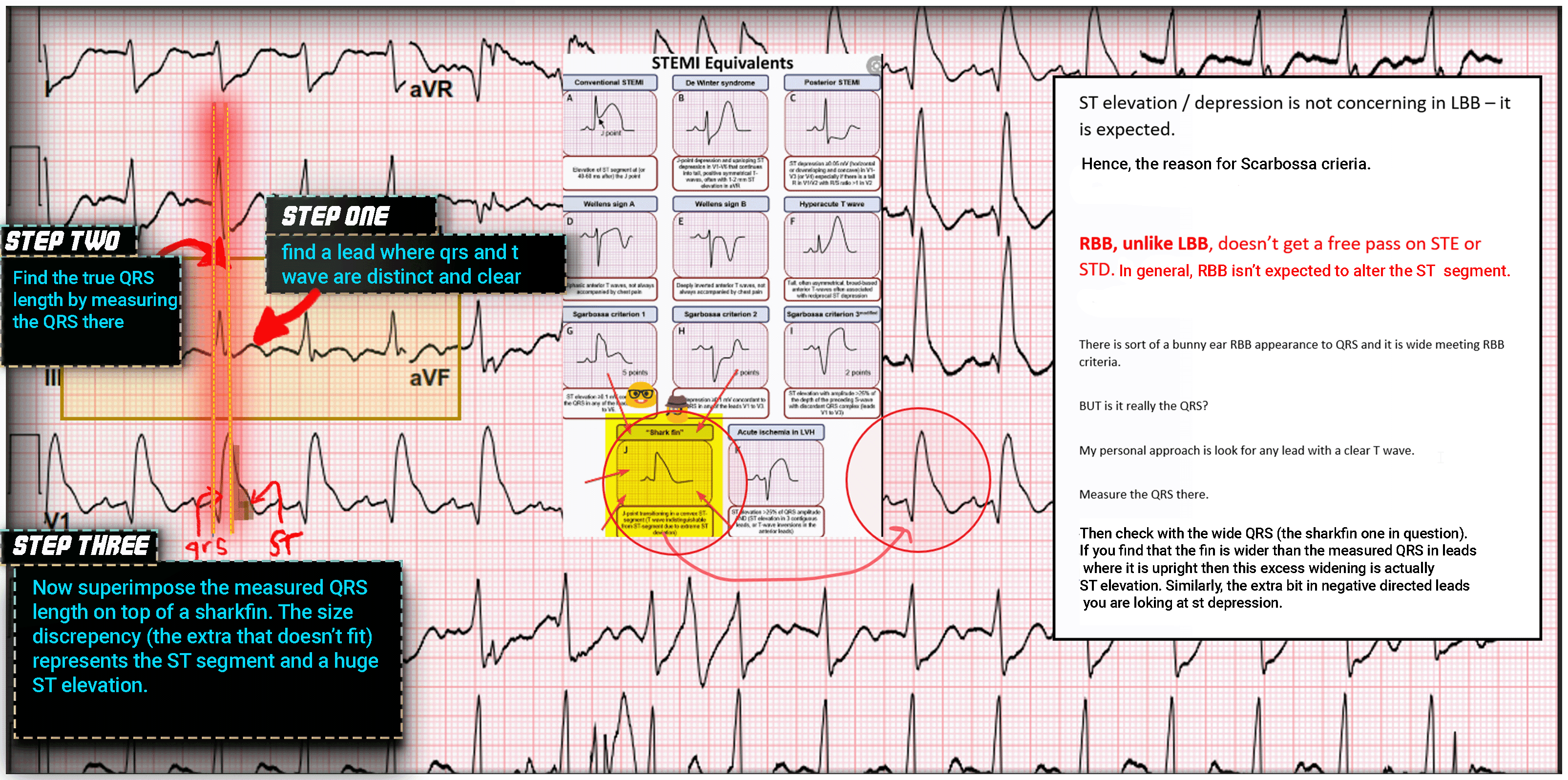
Steps to prove not a right bundle branch block and ST elevation. (Click to enlarge. ESC to return).


Sharkfin
TLDR
There is a tricky situation where massive ST elevation can lead to an unclearly defined ST segment. This can EASILY be mistaken for a RBB by computer and physician alike. Best described as a "sharkfin" appearance the diagnosis is further aided by a technique where segments in well differentiated leads can be measured then superimposed on a sharkfin to reveal it's true colors.
Easy to miss. Impossible to forget.
This is an ecg pattern that you have to have exposure to because it will invariably swim into your ED one day and you can bet money the computer read of the tracing will do it's best to reassure you that it's nothing to worry about. Lets take a quick look at the case.
First the baseline ecg from a few weeks ago. Click to enlarge. ESC to return.
Hidden in plain sight
Patient presented to the ED and coded shortly afterwards. Lets have a look at all the ecg tracings in sequence before discussing them in too much detail. While looking over use this checklist:
1 . Where is the shark fin?
In simple terms explain why this is not a RBB and is STEMI.
A second tracing captured a minute after the first. (Click to enlarge. ESC to return.)
Initial ECG. Pt quickly coded upon entering the ED. (Click to enlarge. ESC to return.)
A final tracing obtained some hours after tpa administration. (Click to enlarge. ESC to return.)
Sharkfin Soup
When facing an odd looking RBB consider STEMI. Also consider hyperkalemia or in some situations VT as well. Also notice how the computer does it's best to reassure you that nothing is the matter here. This is the case in all the cases I have had or those shown to me by colleagues.
Although the RBB in these ecgs might feel a little "off" you really need to be able to clearly and simply explain it to a colleague, the interventionalist, or with enough confidence to pull the trigger on lytics as in this case. Just recognizing something is off about the pattern can be helpful but it is even more helpful to use a tried and true method.
Below is is the strategy I have come up with that best works and I have seen the same described on various other websites—if there is any other tricks please leave a comment so I can learn them.
Steps to prove not a right bundle branch block and ST elevation. (Click to enlarge. ESC to return).