The Upside Down

TLDR
Make sure aVL never becomes your "forgotten lead." This case shows how challenging ecgs can become cakewalk when aVL aids you. This trusty lead often points the direction to ischemia as well as prognosticates. At the conclusion, a mystery of two seemingly incompatible lesion locations on serial ecgs can be understood after the cath report and a little perspective.
TLDR
Make sure aVL never becomes your "forgotten lead." This case shows how challenging ecgs can become cakewalk when aVL aids you. This trusty lead often points the direction to ischemia as well as prognosticates. At the conclusion, a mystery of two seemingly incompatible lesion locations on serial ecgs can be understood after the cath report and a little perspective.

Possible hyperacute T waves in precordial leads alongside ischemic inferolateral changes. Click to open. ESC to close.
An ECG sent to me for read the other night. A couple things stood out.
Precordial leads: T wave symmetry V2-V5. Also ST segment depression and flattening best seen in V5.
III: STEMI-like morphology of ST segment which had extreme flattening with subtle elevation. Although subtle very ischemic appearing shape to ST segment. In addition when the elevation is looked at in terms of proportionality to size of the tiny QRS— any elevation at all is significant.
I and aVL: st depression.
III and aVF: T wave inverted, t wave symmetry
Immediately the precordial T wave morphology jumped out as possibly being "shady" or hyperacute and then the inferior changes. I would have questioned the inferior changes more if it were not for the high lateral changes especially in aVL.
Now I didn't have this patient in front of me, however, I did have an older ecg just a few hours old. So we can take a look at that right below here.
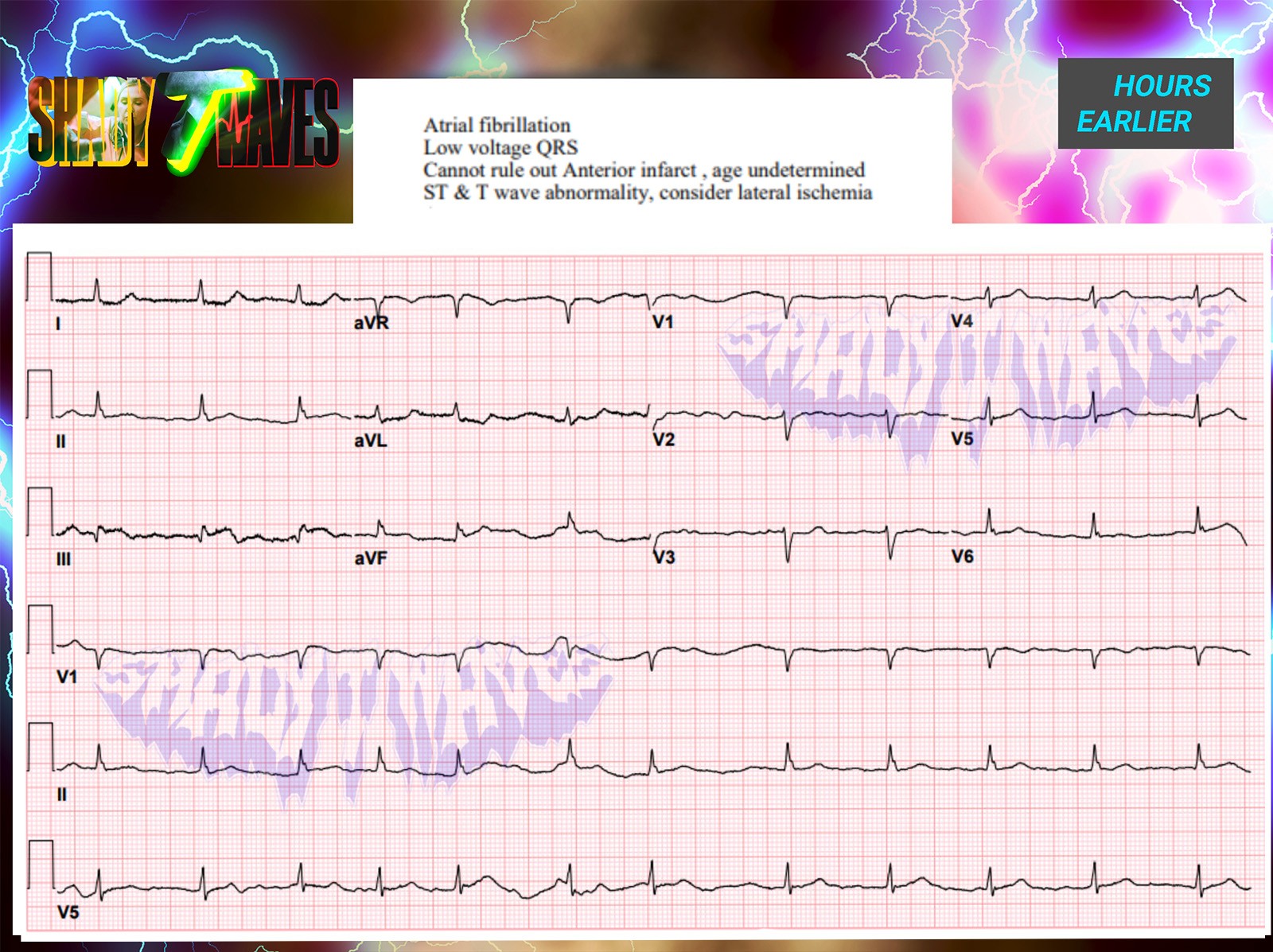
Obtained hours prior, concerning for inferior STEMI. Note how helpful the ST depression and T wave inversion in aVL is in confirming diagnosis given the wandering baseline/artifact in aVF and low amplitude in the inferior leads. Click to open. ESC to close.
Bad to badder
I'd expected a nice looking baseline non ischemic ecg but instead got an even worse ECG. Forget finding confidence for a hyperacute anterior MI—this was diagnostic of inferior STEMI all on it's own without comparison to priors or the newest ecg.
Here's my stepwise thought process in the exact same order as I read it:
Lead III is straight nasty.
Q wave is absolutely massive when looked at proportionally to the rest of the QRS. For example in the first beat the Q wave is as big as the entire complex!
Classic STEMI ST segment morphology. The elevation here is also proportionally huge when compared to the QRS.
While lead III was screaming for a cath I went searching for it's contiguous friend. We have enough for a cath already between the two ecgs. For completeness, this is why I think inferior stemi. Lead III, while a bit shady and hyperacute on the second beat, just takes a little too much imagination at least for me and my current ecg skill level to count.
On the other hand: aVF can fit the bill.
Some artifact complicates the read slightly here but I believe some elevation to be there in addition to some flattening.
No matter what: nobody can argue that proportionally significant ST elevation can be ruled out here. Call it artifact and get a repeat , fine, but you can't dismiss it it the way it looks. Now if you don't see it, that's fine. I'm okay putting a pin on the topic so long as you at least can agree that it can't be fully ruled out.
And this brings me to what is now maybe the forgotten lead. When I trained just a few years ago it was aVR! However, it seems like since, thanks to those foamed masters out there like Smith, Mattu, etc. it may be one of the most well known leads today. I'll hear it talked about even when missing the associated widespread ST depression that is pretty much a prerequisite for concern. We can't help but look at aVR always now. Meanwhile, aVL has now become the forgotten lead in my opinion. That's a shame too because in times of uncertainty it is the best supporting lead and there to crush any doubt. Lets talk more below about our $$ lead aVL.
Best supporting lead goes to….
All hail aVL. The ST changes in aVL should always be looked at very carefully because it can take a non-diagnostic ECG to a diagnostic one. A quick review:
aVL helps identify STEMI in a bunch of places like a boss:
1) Inferior MI
Sensitivity for diagnosis is greatly increased if aVL ST depression and TWI seen alongside inferior ST elevations.
2) RV MI
ST depression >1mm and TWI in aVL: RV involvement in acute inferior MI.
3) Diagonal/high lateral MI
In the case of isolated occlusion of diagonal vessel, or "high lateral MI," ST elevation may only be present in two leads, I and aVL, making the lead essential for diagnosis. (Lead III may aid also with reciprocal depression. )
So we know it more than pulls it's weight. But wait, there's still more reasons to be super super careful when reading an ecg and spend plenty of time on aVL to get it right:
ST depression in aVL with TW inversion also is a huge aid with prognostication of MI:
1) Anterior MI: Ominous finding which is indicative of a more proximal lesion in LAD. Increased risk of badness such as cardiogenic shock, arrythmia.
2) Inferior MI: Worse prognosis and suggestive of more proximal RCA lesion and potential for RV branch involvement. Similarly increased risks.
Be prepared by keeping an eye on this lead.
Curveball to Epiphany
So I think if you can have a little faith in aVL you'll see how diagnostic these ecgs are even if arguing about miniscule millimeters or artifact. You know, I still haven't seen once a tricky ecg case that was cracked by superior measurement skills or missed by a lack of ruler precision yet.
It's a clinical diagnosis not a trigonometry exam.
The faster you can learn to put strict rigid measurement on the backburner and focus on just the shape and contours of each ST segment or T wave the better. You must do this first with every tracing. Ask are the T waves symmetrical, asymmetrical? Is the st segment scooped or flattened, or down sloping or sharp pointed or biphasic? This is far more important than absolute measurement. Sure you can have your time to measure but nothing can ever be measured in isolation. It is an absolute requirement for you to have already calculated your pre -measurement probability of badness for each lead.
If a patient presents with a new flattened ST segment with a massive pathologic Q wave and nearby reciprocal changes and looks like he's about to code then my mental ruler is suddenly looking extremely generous. Not to mention even if my ruler isn't in as generous mood always always do changes need to be appreciated in a proportional sense between QRS and ST segment. Missed cases happen more often I find because we miss the other sign posts, like our buddy aVL, or get misdirected by negative labs, missing history, missing prior tracings, or anchor on atypical symptoms. If there are some missed by measurement I promise you that if the person had just looked at the st segment in a proportional way they would have caught it. It's easier than measuring too!
So I said it's a clinical diagnosis, right? I get ready to call the cardiologist but first make a call up to the patient's room. As I'm waiting a brief second I see the lab results. Initial troponin wnl. A second one in progress.
I ask RN how are they feeling what symptoms do they have? "They're great , she said." They haven't had a single symptom at all since I started my shift.
"Okay, then what prompted this ecg?" I ask. "We just got a call from the lab that the troponin was high I think they're trying to get ahold of the provider now to tell them. That's why I did it , but she feels great now."
I still talked to the cardiology team. But, I felt at the time like I was thrown a curve ball. I'd expect those to be hyperacute t waves in the anterior leads and with the confirmed inferior changes and them being asymptomatic it didn't add up quite right to me.
Ultimately, it turned out the curveball I was thrown was a bone and made sense of the entire case. I didn't realize it until later at home.
I won't lie to you…I didn't put it all together until after waking up later that evening when reading the interventions on the cath report.
1.Mid portion of posterolateral branch received stent x 1. They remarked at time of cath was 85% stenosis and not fully occluded and also with evidence of embolization to adjacent distal PL branch.
Ostial (proximal) RCA with apparent plaque disruption vs. dissection received 2 x stent.
They weren't hyperacute T waves. After all she was asymptomatic, right. The clue was right there all along. She was asymptomatic, felt great, something changed. The confirmation of inferior MI and disrupted embolized plaque in the posterior lateral branch proves these upright symmetric t waves were significant but not for the reasons I thought. They were showing a window to the posterior heart and must be flipped/mirrored to see their true identity: our trusty reperfusion waves. I know we aren't talking about the LAD but they're still a "wellenish" wave of the type b category. If flipped in our minds when looking at the tracing we are now seeing symmetric deep t wave inversions in the anterior leads, consistent with improved symptoms, and reperfusion which is verified on the cath report as evidently rupturing and embolizing distally—thus reperfusion on the branch.
At least that is my unifying theory. If I missed something or you think I'm way off let me know or if I missed some other clues seen along the way.
For more, I recommend reading:
Dr. Smith's ECG Blog : March 6th 2023 Post
https://hqmeded-ecg.blogspot.com/2023/03/what-do-you-think-of-this-ecg-is-this.html
Comments

The Upside Down
TLDR
Make sure aVL never becomes your "forgotten lead." This case shows how challenging ecgs can become cakewalk when aVL aids you. This trusty lead often points the direction to ischemia as well as prognosticates. At the conclusion, a mystery of two seemingly incompatible lesion locations on serial ecgs can be understood after the cath report and a little perspective.
Possible hyperacute T waves in precordial leads alongside ischemic inferolateral changes. Click to open. ESC to close.
An ECG sent to me for read the other night. A couple things stood out.
Precordial leads: T wave symmetry V2-V5. Also ST segment depression and flattening best seen in V5.
III: STEMI-like morphology of ST segment which had extreme flattening with subtle elevation. Although subtle very ischemic appearing shape to ST segment. In addition when the elevation is looked at in terms of proportionality to size of the tiny QRS— any elevation at all is significant.
I and aVL: st depression.
III and aVF: T wave inverted, t wave symmetry
Immediately the precordial T wave morphology jumped out as possibly being "shady" or hyperacute and then the inferior changes. I would have questioned the inferior changes more if it were not for the high lateral changes especially in aVL.
Now I didn't have this patient in front of me, however, I did have an older ecg just a few hours old. So we can take a look at that right below here.
Obtained hours prior, concerning for inferior STEMI. Note how helpful the ST depression and T wave inversion in aVL is in confirming diagnosis given the wandering baseline/artifact in aVF and low amplitude in the inferior leads. Click to open. ESC to close.
Bad to badder
I'd expected a nice looking baseline non ischemic ecg but instead got an even worse ECG. Forget finding confidence for a hyperacute anterior MI—this was diagnostic of inferior STEMI all on it's own without comparison to priors or the newest ecg.
Here's my stepwise thought process in the exact same order as I read it:
Lead III is straight nasty.
Q wave is absolutely massive when looked at proportionally to the rest of the QRS. For example in the first beat the Q wave is as big as the entire complex!
Classic STEMI ST segment morphology. The elevation here is also proportionally huge when compared to the QRS.
While lead III was screaming for a cath I went searching for it's contiguous friend. We have enough for a cath already between the two ecgs. For completeness, this is why I think inferior stemi. Lead III, while a bit shady and hyperacute on the second beat, just takes a little too much imagination at least for me and my current ecg skill level to count.
On the other hand: aVF can fit the bill.
Some artifact complicates the read slightly here but I believe some elevation to be there in addition to some flattening.
No matter what: nobody can argue that proportionally significant ST elevation can be ruled out here. Call it artifact and get a repeat , fine, but you can't dismiss it it the way it looks. Now if you don't see it, that's fine. I'm okay putting a pin on the topic so long as you at least can agree that it can't be fully ruled out.
And this brings me to what is now maybe the forgotten lead. When I trained just a few years ago it was aVR! However, it seems like since, thanks to those foamed masters out there like Smith, Mattu, etc. it may be one of the most well known leads today. I'll hear it talked about even when missing the associated widespread ST depression that is pretty much a prerequisite for concern. We can't help but look at aVR always now. Meanwhile, aVL has now become the forgotten lead in my opinion. That's a shame too because in times of uncertainty it is the best supporting lead and there to crush any doubt. Lets talk more below about our $$ lead aVL.
Best supporting lead goes to….
All hail aVL. The ST changes in aVL should always be looked at very carefully because it can take a non-diagnostic ECG to a diagnostic one. A quick review:
aVL helps identify STEMI in a bunch of places like a boss:
1) Inferior MI
Sensitivity for diagnosis is greatly increased if aVL ST depression and TWI seen alongside inferior ST elevations.
2) RV MI
ST depression >1mm and TWI in aVL: RV involvement in acute inferior MI.
3) Diagonal/high lateral MI
In the case of isolated occlusion of diagonal vessel, or "high lateral MI," ST elevation may only be present in two leads, I and aVL, making the lead essential for diagnosis. (Lead III may aid also with reciprocal depression. )
So we know it more than pulls it's weight. But wait, there's still more reasons to be super super careful when reading an ecg and spend plenty of time on aVL to get it right:
ST depression in aVL with TW inversion also is a huge aid with prognostication of MI:
1) Anterior MI: Ominous finding which is indicative of a more proximal lesion in LAD. Increased risk of badness such as cardiogenic shock, arrythmia.
2) Inferior MI: Worse prognosis and suggestive of more proximal RCA lesion and potential for RV branch involvement. Similarly increased risks.
Be prepared by keeping an eye on this lead.
Curveball to Epiphany
So I think if you can have a little faith in aVL you'll see how diagnostic these ecgs are even if arguing about miniscule millimeters or artifact. You know, I still haven't seen once a tricky ecg case that was cracked by superior measurement skills or missed by a lack of ruler precision yet.
It's a clinical diagnosis not a trigonometry exam.
The faster you can learn to put strict rigid measurement on the backburner and focus on just the shape and contours of each ST segment or T wave the better. You must do this first with every tracing. Ask are the T waves symmetrical, asymmetrical? Is the st segment scooped or flattened, or down sloping or sharp pointed or biphasic? This is far more important than absolute measurement. Sure you can have your time to measure but nothing can ever be measured in isolation. It is an absolute requirement for you to have already calculated your pre -measurement probability of badness for each lead.
If a patient presents with a new flattened ST segment with a massive pathologic Q wave and nearby reciprocal changes and looks like he's about to code then my mental ruler is suddenly looking extremely generous. Not to mention even if my ruler isn't in as generous mood always always do changes need to be appreciated in a proportional sense between QRS and ST segment. Missed cases happen more often I find because we miss the other sign posts, like our buddy aVL, or get misdirected by negative labs, missing history, missing prior tracings, or anchor on atypical symptoms. If there are some missed by measurement I promise you that if the person had just looked at the st segment in a proportional way they would have caught it. It's easier than measuring too!
So I said it's a clinical diagnosis, right? I get ready to call the cardiologist but first make a call up to the patient's room. As I'm waiting a brief second I see the lab results. Initial troponin wnl. A second one in progress.
I ask RN how are they feeling what symptoms do they have? "They're great , she said." They haven't had a single symptom at all since I started my shift.
"Okay, then what prompted this ecg?" I ask. "We just got a call from the lab that the troponin was high I think they're trying to get ahold of the provider now to tell them. That's why I did it , but she feels great now."
I still talked to the cardiology team. But, I felt at the time like I was thrown a curve ball. I'd expect those to be hyperacute t waves in the anterior leads and with the confirmed inferior changes and them being asymptomatic it didn't add up quite right to me.
Ultimately, it turned out the curveball I was thrown was a bone and made sense of the entire case. I didn't realize it until later at home.
I won't lie to you…I didn't put it all together until after waking up later that evening when reading the interventions on the cath report.
1.Mid portion of posterolateral branch received stent x 1. They remarked at time of cath was 85% stenosis and not fully occluded and also with evidence of embolization to adjacent distal PL branch.
Ostial (proximal) RCA with apparent plaque disruption vs. dissection received 2 x stent.
They weren't hyperacute T waves. After all she was asymptomatic, right. The clue was right there all along. She was asymptomatic, felt great, something changed. The confirmation of inferior MI and disrupted embolized plaque in the posterior lateral branch proves these upright symmetric t waves were significant but not for the reasons I thought. They were showing a window to the posterior heart and must be flipped/mirrored to see their true identity: our trusty reperfusion waves. I know we aren't talking about the LAD but they're still a "wellenish" wave of the type b category. If flipped in our minds when looking at the tracing we are now seeing symmetric deep t wave inversions in the anterior leads, consistent with improved symptoms, and reperfusion which is verified on the cath report as evidently rupturing and embolizing distally—thus reperfusion on the branch.
At least that is my unifying theory. If I missed something or you think I'm way off let me know or if I missed some other clues seen along the way.
For more, I recommend reading:
Dr. Smith's ECG Blog : March 6th 2023 Post
https://hqmeded-ecg.blogspot.com/2023/03/what-do-you-think-of-this-ecg-is-this.html
Comments